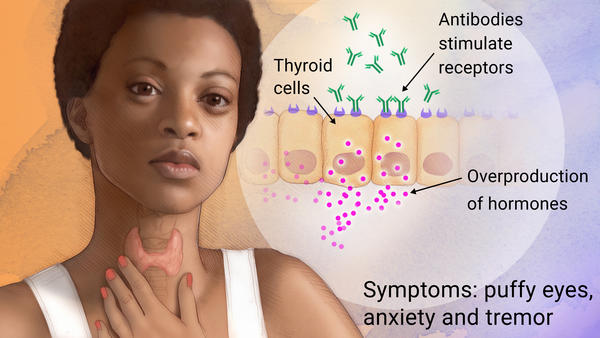
Graves' disease is an autoimmune disease in which the overactivity of the thyroid gland causes the overproduction of thyroid hormones (hyperthyroidism).
A number of conditions can cause hyperthyroidism, but Graves' disease is the most common.
The disease can affect adolescents and is most often diagnosed among women under 40 years old, but can also be found in men.
If left untreated, Graves' disease can have a major negative impact on a person's mental and physical state.
Requires a medical diagnosis.
Symptoms include anxiety, hand tremor, heat sensitivity, weight loss, puffy eyes and enlarged thyroid.
People may experience:
Whole body: excess sweating, fatigue, heat intolerance, or high blood pressure
Heart: fast heart rate, irregular heart rate, or palpitations
Eyes: abnormal protrusion of eyes or puffy eyes
Also common: absence of menstruation, anxiety, diarrhoea, enlarged thyroid, hair loss, hand tremor, insomnia, irritability, muscle weakness, nervousness, puffy skin changes on the shin, or weight loss
Here are some key points on Graves' disease.
A number of conditions can cause hyperthyroidism, but Graves' disease is the most common.
The disease can affect adolescents and is most often diagnosed among women under 40 years old, but can also be found in men.
If left untreated, Graves' disease can have a major negative impact on a person's mental and physical state.
Requires a medical diagnosis.
Symptoms include anxiety, hand tremor, heat sensitivity, weight loss, puffy eyes and enlarged thyroid.
People may experience:
Whole body: excess sweating, fatigue, heat intolerance, or high blood pressure
Heart: fast heart rate, irregular heart rate, or palpitations
Eyes: abnormal protrusion of eyes or puffy eyes
Also common: absence of menstruation, anxiety, diarrhoea, enlarged thyroid, hair loss, hand tremor, insomnia, irritability, muscle weakness, nervousness, puffy skin changes on the shin, or weight loss
Here are some key points on Graves' disease.
- Graves' disease is the most common cause of hyperthyroidism.
- The disease is also the most common type autoimmune disease in the US.
- It is more common in women under the age of 40, but can also be found in men.
- Graves' disease affects an estimated 2-3% of the world's population.
- The disease can be passed down through families, but its inheritance patterns remain unclear.
- The disease is named after Sir Robert Graves, an Irish Doctor, who first described the condition in 183